Methylphenidate (Ritalin)-Induced Proteinuria: A Case Report of a Teenager with Reversible Renal Side Effects
Dr. Gita Sharifi
Lab, licensed by Shahid Beheshti University of Medical Sciences, Department of Clinical Laboratory Sciences, Tehran, Iran
APFCB News Volume 5, Issue 1
Introduction
Proteinuria, defined as the presence of abnormal amounts of protein in the urine (usually more than 150 mg/24 hours), is a common laboratory finding that reflects abnormal permeability of the glomerular filtration barrier, which may result from a variety of renal and systemic conditions.[1] The causes of proteinuria range from benign transient conditions to serious glomerular diseases and include glomerular, tubular, overflow, and functional (transient)proteinuria. While glomerular diseases represent the most common causes for proteinuria, Drug-induced proteinuria is also recognized, with several medications (like NSAIDS, ACE inhibitors, some Antibiotics such as aminoglycosides) implicated in renal injury either by direct nephrotoxic effects or by altering renal hemodynamic.[4,5] Methylphenidate, commonly known as Ritalin, is a CNS(Central Nervous System) stimulant widely prescribed for the treatment of ADHD (Attention-Deficit Hyperactivity Disorder). While its cardiovascular, gastrointestinal, and neuropsychiatric complications are well documented, reports of its renal side effects are exceedingly rare.[2] However, emerging evidence suggests that Methylphenidate may affect renal function, potentially leading to proteinuria.[3] Although the exact incidence and clinical significance remain unclear, this case report highlights a rare but noteworthy association between Methylphenidate use and abnormal urinary protein excretion.[6]
Case Presentation
This case report describes a high school student with no physical history of renal disorder, 1 year, without evidence of vesicoureteral reflux as confirmed by VCUG (Voiding Cystourethrogram).
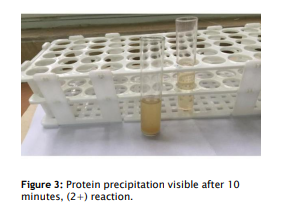
This female student was initially prescribed Ritalin 10 mg twice daily (morning and afternoon) in primary school due to suspected attention deficit, though symptoms did not persist and medication was soon stopped without adverse effects. During high school, she resumed Ritalin use occasionally before exams, under medical supervision. At age 15 y, she took the medication 10mg once daily for a month, after which routine urinalysis showed mild (trace) proteinuria. The following year, after one week of similar Ritalin use, she developed marked proteinuria (2+ in qualitative method),meaning that laboratory analysis using the sulfosalicylic acid (3%) turbidimetric method confirmed high urinary protein.(Figures 1 to 3). Biochemistry autoanalyzer results revealed a random urine protein concentration of 1739 mg/L (reference range: 14–141 mg/L). After stopping the treatment, a follow-up 24-hour urine test showed 161.2 mg/24hr (normal: up to 150 mg/24hr), indicating improvement after discontinuation of the medicine.
She permanently ceased Ritalin use thereafter, with no recurrence of proteinuria.[2,3]
Figures: Actual photos of the case, showing sulfosalicylic acid precipitation reaction.
Random urine supernatant after centrifuging (right) and precipitation with sulfosalicylic acid (left). (Qualitative method for evaluating the amount of proteinuria)

Discussion
To date, reports of proteinuria directly associated with Methylphenidate use are exceedingly rare in the medical literature.[3] While several cases of complications have been documented in patients receiving Methylphenidate, explicit documentation of proteinuria as a presenting feature is limited. This scarcity underscores the novelty and clinical significance of the present case. Reporting such uncommon adverse effects is crucial to raise awareness among clinicians about the potential renal implications of stimulant medications. Given the increasing prevalence of Methylphenidate use worldwide, especially in pediatric and adult ADHD populations, more vigilance and investigation into its renal safety profile and probable side effects and their mechanisms are warranted for further studies.
Methylphenidate, through its stimulation of the sympathetic nervous system and increased release of catecholamines such as norepinephrine and dopamine, places the body in a heightened state of physiological stress. This adrenergic surge can lead to vasoconstriction, elevated blood pressure, and altered renal hemodynamics.[6] Such changes potentially reduce renal perfusion and glomerular filtration rate, predisposing renal cells to ischemic stress. Cellular stress induced by hypoperfusion and oxidative stress may activate apoptotic pathways, leading to programmed cell death (apoptosis) in glomerular and tubular cells.[7,8] While direct cytotoxic effects of Methylphenidate on renal cells have not been definitively demonstrated, these indirect mechanisms suggest a plausible pathway for Methylphenidate-associated proteinuria via injury to the renal filtration barrier. Further research is necessary to elucidate the extent and clinical significance of these effects.
Hence, the underlying mechanism by which Methylphenidate (Ritalin) may induce proteinuria is not yet fully understood and remains speculative, but experimental studies have also suggested that Methylphenidate can reduce glomerular filtration rate and alter sodium handling, possibly due to renal vasoconstriction or sympathetic nervous system overactivation.[6,8] These hemodynamic changes may lead to transient glomerular injury, predisposing patients to proteinuria.
This case report emphasizes the importance of a comprehensive and detailed clinical assessment, including medication history, when evaluating patients with unexplained proteinuria, and identifying potential drug-induced causes is crucial for appropriate management and may prevent unnecessary diagnostic procedures.
Finally, although Ritalin is not typically associated with renal side effects, this case indicates a temporal relationship between Ritalin consumption and transient proteinuria. Further studies are needed to elucidate the potential nephrotoxic effects of Methylphenidate and their clinical implications. It is suggested that the next studies investigate the potential renal side effects of Methylphenidate, particularly its possible association with proteinuria. Moreover, further research is warranted to clarify whether such adverse effects may be more relevant in female children with a history of urinary tract infection.
Conclusion
In conclusion, this case report highlights a rare but important association between Methylphenidate use and the development of proteinuria. Although the precise mechanisms remain to be fully elucidated, possible hemodynamic alterations and cellular stress induced by sympathetic stimulation may play a role in renal injury. Clinicians should maintain a high index of suspicion for drug-induced renal effects when evaluating unexplained proteinuria, particularly in patients receiving stimulant medications. Methylphenidate is metabolized in the liver and primarily excreted via the kidneys, which may contribute to its potential renal effects, including proteinuria.(2,3,6) Further research is needed to clarify the underlying pathophysiology and to guide optimal management and monitoring strategies for affected individuals.As a result, Clinicians should be aware of the possibility of proteinuria as a rare side effect of Ritalin.[8,10] Monitoring urinary findings during prolonged or repeated use, especially in adolescents, may be prudent.[8,9]
Funding: None declared
Conflict of Interest
The author declares no conflicts of interest. All of the tests were done in the author’s Medical Lab.
References:
1. Glassock RJ, Cohen AH, Adler SG. Primary glomerular diseases. In: Taal MW, Chertow GM, Marsden PA, Skorecki K, Yu ASL, Brenner BM, editors. Brenner and Rector's The Kidney. 10th ed. Philadelphia: Elsevier; 2016. p. 1100-1250.
2. Kollins SH. Pharmacokinetic and pharmacodynamic profile of methylphenidate in humans. Pharmacol Biochem Behav. 2003;76(2):341-347. doi:10.1016/S0091-3057(03)00213-6
3. Shafa Sh, Khosravi M, Ghaffari S. Study of the safety of methylphenidate: Focus on nephrotoxicity aspects. Life Sci. 2015;141:137-142. doi:10.1016/j.lfs.2015.09.014
4. Perazella MA. Drug-induced nephropathy: an update. Expert Opin Drug Saf. 2005;4(4):689- 706. doi:10.1517/14740338.4.4.689
5. Izzedine H, Perazella MA. Anticancer drug-induced acute kidney injury. Kidney Int Rep. 2017;2(4):504-514. doi:10.1016/j.ekir.2017.02.009
6. Perazella MA. Pharmacology behind common drug nephrotoxicities. Clin J Am Soc Nephrol. 2018;13(12):1897-1908. doi:10.2215/CJN.00150118
7. Stevens PE, Levin A. Evaluation and management of chronic kidney disease: KDIGO 2012 Clinical Practice Guideline. Kidney Int Suppl. 2013;3(1):1-150. doi:10.1038/kisup.2012.73
8. Perazella MA, Rosner MH. Drug-induced proteinuria: mechanisms and clinical relevance. Nat Rev Nephrol. 2014;10(9):517-530. doi:10.1038/nrneph.2014.113
9. Upadhyay A, Earley A, Haynes SM, Uhlig K. Systematic review: blood pressure target in chronic kidney disease and proteinuria as an effect modifier. Ann Intern Med. 2011;154(8):541-548. doi:10.7326/0003-4819-154-8-201104190-00335 10. Davison AM, Cameron JS, Grünfeld JP, Kerr DN, Ritz E, Winearls CG, editors. Oxford Textbook of Clinical Nephrology. 4th ed. Oxford: Oxford University Press; 2016.
